
OUR CHILDREN - CDC'S PAWNS
OUR CHILDREN - CDC'S PAWNS
When The Thirst for Power and Money Replaces Public Health

“Preventing COVID-19 among children and teens is important to slow the spread of SARS-CoV-2, the virus that causes COVID-19, and protect them from severe illness.”
”CDC recommends that everyone ages 5 years and older get their primary series of COVID-19 vaccine, and everyone ages 12 years and older also receive a booster.”
Looking at these two sentences from the most prestigious public health agency in the Universe I can only conclude that 1) our children and teens are suffering a disproportionate amount of severe illness following a SARS-CoV-2 infection (COVID-19) AND 2) having children and teens “vaccinated” and boosted will stop that infection in its tracks.
Let’s take a look at the data upon which CDC is basing this recommendation. First a word about “severe illness”. I have said from the first day that the world began talking about SARS-CoV-2 and COVID-19 that the only outcome of concern was mortality but since we’re discussing “severe illness” let’s also look at hospitalizations. After all, there is no better sign of a “sever illness” than a hospital admission.
New hospitalizations among children and teens 0-17 years of age in the US peaked during the Omicron surge and reached a peak rate of 1.24 new admissions/100,000 population. According to Statisa.com there are approximately 73,000,000 children between the ages of 0-17 years in the United States. That means that at the PEAK of of the Omicron surge there were about 905.2 children and teens who became severely ill enough to be admitted to the hospital; 905.2 in all of the United States.

But what about mortality - the ultimate measure of “severe illness”?
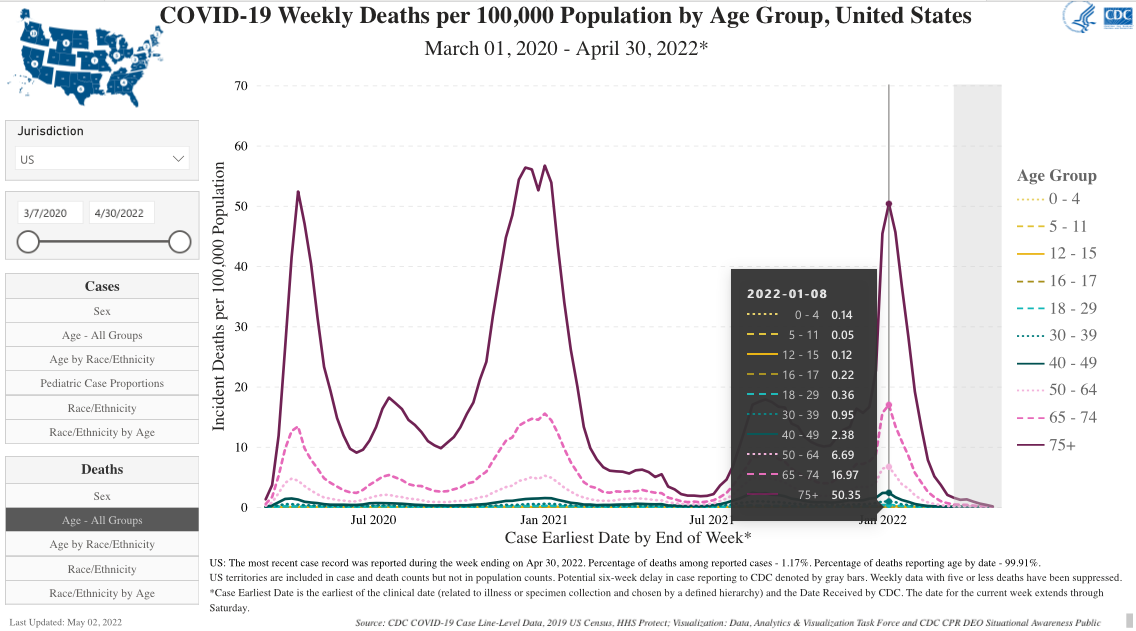
As the following graph shows, through out the ENTIRE “pandemic” 0.53 children 0-17 years of age/100,000 of population died WITH COVID-19 (remember about 94% of all COVID-19 attributed deaths occurred among people who were in extremely poor health). Again, based on 73 million children and teens 0-17 years of age, 0.053/100,000 means that in the entire United States about 386.9 of them died.
CDC offers no insight concerning the overlap among those who were admitted to the hospital and those who died but for the sake of argument and to help CDC build its case, I’ll assume that they are wholly separate groups which at their worst experience period 1,289.1 children and teens between 0 and 17 years of age suffered an illness severe enough to either hospitalize or kill them which equates to 0.0018% of the entire demographic.
It is upon this data the Rochelle Walensky’s CDC is “recommending that you “vaccinate” your children. By the way, the use of “recommendation” by CDC is highly unusual. Historically, CDC has viewed “recommendation” as a regulatory word and thus they have stayed away from it use, preferring the “non-regulatory” word “guideline”. Apparently, Rochelle Walensky is a bit more dogmatic than all of her predecessors.
So let’s say that you are convinced, compelled, obligated to vaccinate your children based on this CDC recommendation. CDC has insisted that the mRNA stuff they call a vaccine is safe and effective but in not preventing the spread of SARS-CoV-2 only in reducing a “severe illness” — like death.
Enter Spiro P. Pantazatos and his colleague Herve’ Seligmann authors of COVID vaccination and age-stratified all-cause mortality risk. Pantazatos and Seligmann compared their estimates of Vaccine-induced Fatality Rates (VFR) to CDC’s estimates contained in its Vaccine Adverse Effects Report System (VAERS). While CDC relied on reports of VFR from VAERS but did not consider the well established under reporting associated with the system, Pantazatos and Seligmann used “two independent, publicly available data sources from the USS and Europe”.
Pantazatos and Seligmann found that children between the ages of 0 and 17 had a Vaccine-induced Fatality Rate of 0.04% which is 20 times greater than the CDC VFR (based on VAERS) of 0.002%.
If you are a regular reader of this Newsletter you may have read my piece on Bell’s Palsy in children following injection of the mRNA stuff as well as my Newsletters on Myo/peridarditis in teens and young people.
Here is what Pantazatos and Seligmann wrote in their section, Implications for public health policy:
“Given that vaccines do not appear to reduce community spread and that the risks out weigh the benefits for most age groups, vaccine mandates in workplaces, colleges, schools and elsewhere are ill-advised. We do not see much benefit in vaccine mandates other than increasing serviceable obtainable market (SOM) share for the vaccine companies.”
There is not a single bit of data in CDC’s possession to suggest that the “vaccination” of children and teens is necessary — for any purpose. On the other hand there is every reason not to inject them.
10 “See that you do not despise one of these little ones. For I tell you that in heaven their angels always see the face of my Father who is in heaven….” Matthew 18:10
Union, KY
3 May 2022
[
VFR is 0.0002% per CDC. Covid fatality rate in 0-17 is 0.54/100k, or 0.0005%. Thats a FR that is 2.5 times CDC admitted VFR. Thats grounds right there for rejection if the Covid fatality rate number is correct